Cognitive impairment can be caused by a variety of things.
~ Vascular Dementia from stroke or impeded blood flow to brain
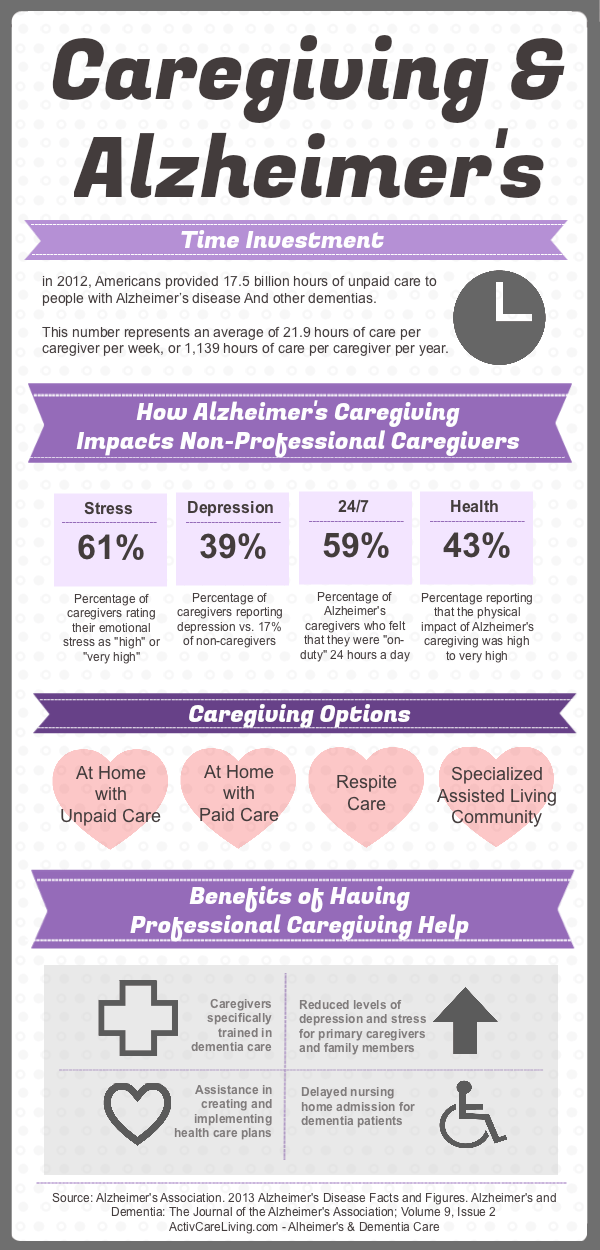
~ Alzheimer's
~ Brain Injury from a fall
~ Primary or secondary brain tumor
~ Endocrine conditions (hypothyroidism, hypercalcemia, hypoglycemia)
~ Nutritional conditions (deficiency of thiamin, niacin, or vitamin b12 (Wernike-Korsakoff’s Syndrome))
~ Infectious conditions (HIV, neurosyphilis, cryptococcus)
~ Problems with renal and hepatic function
~ Effects of medications (e.g., benzodiazepines)
~ The toxic effect of long-standing substance abuse
The mode of onset, subsequent course and reversibility of dementia depend on the underlying etiology
Important Aspects of Management
~ Counselor Goals
~ Establish and maintain an alliance with the patient and family
~ Perform a diagnostic evaluation and refer the patient for any needed general medical care
~ Assess and monitor psychiatric status for the presence of noncognitive psychiatric symptoms and progression of cognitive symptoms.
~ Educate the patient and family about future symptoms and the care likely to be required
~ Help patients and their families think about financial and legal issues due to the patient's incapacity
Important Aspects of Management
~ Counselor Goals
~ Help patients and their families think about financial and legal issues due to the patient's incapacity
~ Educate the patient and family about the illness, its treatment, and available sources of care and support
~ Monitor safety and intervene when required
~ Improving quality of life
~ Maximizing function in the context of existing deficits
~ Improvement of cognitive skills, mood, or behavior
Goals for treatments for cognitive and functional losses include:
~ Restoring cognitive abilities
~ Preventing further decline
~ Increasing functional status
~ Decrease independent agitation, screaming, combativeness
~ Increase the comfort and safety of patients and their families and caregivers
~ Educating patients and families about the illness and treatment, sources of additional care and support (e.g. Support groups, respite care, nursing homes, and other long-term-care facilities), and the need for financial and legal planning due to the patient’s eventual incapacity (e.g. Power of attorney for medical and financial decisions, an up-to-date will, and the cost of long-term care)
Basic principles of care to be remembered by counselors and family include
~ Keeping requests and demands relatively simple and avoiding overly complex tasks that might lead to frustration
~ Avoiding confrontation and deferring requests if the patient becomes angered
~ Remaining calm, firm, and supportive if the patient becomes upset
~ Being consistent and avoiding unnecessary change
~ Providing frequent reminders, explanations, and orientation clues
~ Recognizing declines in capacity and adjusting expectations appropriately
~ Bringing sudden declines in function and the emergence of new symptoms to psychiatrist
~ Behavioral symptoms can be precipitated by both over and understimulation
~ Patients and their families are often dealing with recognition of the illness and associated limitations, and they may appreciate suggestions for how to cope with these limitations (e.g., making lists, using a calendar).
~ It is important to identify specific impairments and highlight remaining abilities.
~ Patients with moderate to severe major depression who do not respond to or cannot tolerate antidepressant medications should be considered for ECT.
Treatment plan for moderately impaired patients should include:
~ Increased supervision
~ Families should be advised regarding the possibility of accidents due to forgetfulness (e.g., fires while cooking), of difficulties coping with household emergencies, and wandering
~ Patients should be strongly urged not to drive
~ As patients' dependency increases, respite care (e.g., home health aid, day care, or brief nursing home stay) may be helpful
~ At this stage, families should begin to consider and plan for additional support at home or possible transfer to a long-term care facility.
~ Delusions and hallucinations often develop in moderately impaired patients.
~ Combativeness, and physical violence are often associated with frustration, misinterpretations, delusions, or hallucinations, and pose a particular problem for patients cared for at home
Handling Troubling Behaviors
~ Try to accommodate the behavior, not control the behavior
~ For example, if the person insists on sleeping on the floor, place a mattress on the floor to make him more comfortable.
~ Remember that we can change our behavior or the physical environment.
~ Changing our own behavior will often result in a change in our loved one’s behavior. (Frustration -> frustration)
~ Check with the doctor first. Behavioral problems may have an underlying medical reason, i.e. pain or experiencing an adverse side effect from medications.
~ Behavior has a purpose. People with dementia typically cannot tell us what they want or need. They might do something, like take all the clothes out of the closet on a daily basis, and we wonder why. Always consider what need the person might be trying to meet with their behavior—and, when possible, try to accommodate them.
~ What works today, may not tomorrow because multiple factors influence troubling behaviors, and there is a natural progression of the disease process
~ The key to managing difficult behaviors is being creative and flexible in your strategies to address a given issue. Behavior is triggered. It occurs for a reason. It might be something a person did or said. It could be a change in the physical environment. The root to changing behavior is disrupting the patterns that we create. Try a different approach, or a different consequence. (Positive redirection).
View the Counseling CEU course for this presentation.
This course is also included in our unlimited CEU packages.